

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
14.11.25/ 5.12.25
These are 4 posts on the topic of “Pleura”. 04 is the first one, addressing the anatomical and physiological basics of the rib and lung pleura, as well as a single pathological change: the pneumothorax. This post is strongly aimed at medical laypeople, unlike the next three posts, which require basic medical knowledge. These three posts are also labeled with the Roman numerals II- IV. They deal with effusions between the pleural layers that do not resolve but become chronic diseases. They are dangerous because the underlying inflammatory disease can often recur here.
Cases 41-45: Effects of Fibrothorax
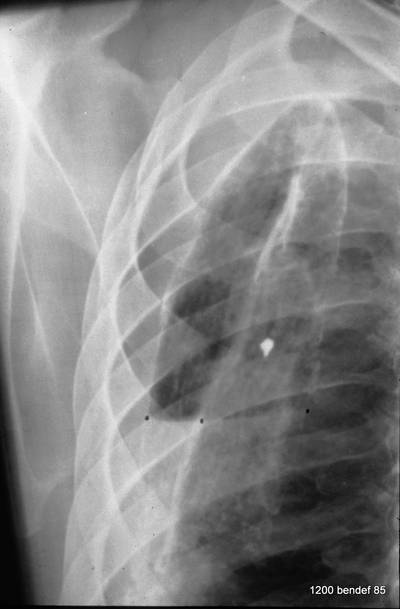
41. Next case. History of left-sided pleural empyema; recently a small pneumonia on the right side.
At first glance: mass in the left hilum? Probably bronchial carcinoma?
Image 41: At first glance: mass in the left hilum? Probably bronchial carcinoma?
Caution! There is another finding; this one is not trivial, although not malignant, but much more serious than many think: calcification at the upper edge of the left lung field.
What should we do next?
In the past, the first idea would have been “fluoroscopy.” However, today we perform a CT scan. – With contrast?
“CT with contrast” answers the question: Is it a vascular structure? Is the tissue being supplied with blood?
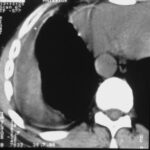
Image 42: Same patient. What do we find in the contrast-enhanced CT?
No tumor, but a marked enlargement of the pulmonary artery. The enlargement of the vessel volume corresponds to the tension of the pleuro-pulmonary scars.
We see a pleural scar in the upper lung field and even a small, persistent effusion between the two calcified pleural layers. –
By the way, the morphological findings of the pulmonary valve function and the pressure in the large vessels were normal.
A new incidental finding is a small right-sided dorsal pleural effusion, probably related to a recent case of pneumonia.
New patient; When thinking of calcified pleura, many assume the disease has healed. Unfortunately, this reflex “calcified pleura = healed disease” is unfounded and can delay the correct diagnosis. (In the following, we see one of the rare cases where pleural calcification hindered the diagnosis.)Image
43: Could the mass be a persistent effusion or fibrous tissue?
Diagnosis: A neoplasm; in this case, it is a peripheral bronchial carcinoma.
The attention was diverted by the pleural finding.
Could the mass be a persistent effusion or fibrous tissue?
No, it is too irregular in shape and too heterogeneous.
Is another tumor possible? Yes, mesothelioma (note the diaphragm calcification, suspicion of asbestosis?).
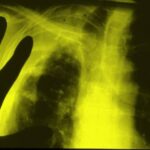
44. “H. E.” He is suffering from acute fever, cough, and elevated CRP. – Fibrothorax for 20 years. You observe signs associated with Fibrothorax.
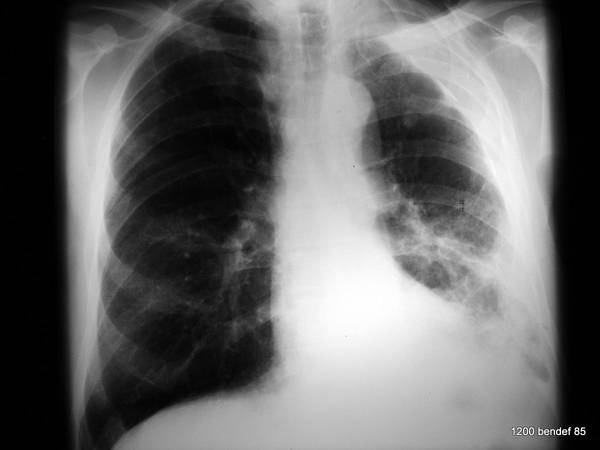
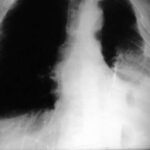
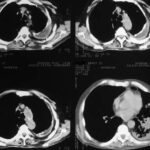
Image 44: “Old” tuberculosis patient. What is your diagnosis?
The “Fibrothorax” with calcified inner and outer edges creates an unusually wide shadow in the left upper and middle fields. Additionally, streaky shadows can be seen in the left lower field.
The next image is part of the CT scan.
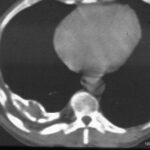
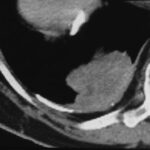
45. The irregular shadow in the left lower lobe is shown in other slices with a positive air bronchogram (representation of the bronchi by their air content and the surrounding tissue consolidation). It is not shown here. A pneumonia is the most likely cause for this sign, especially given the clinical picture.
Image 45: Same patient. What is behind the shadow?
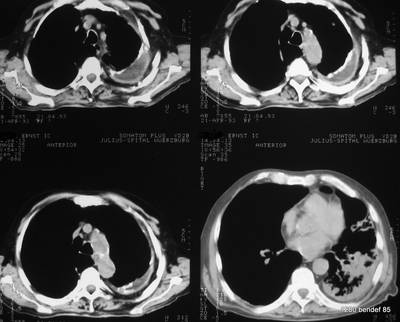
How would you describe the lesion in the upper area of the left thorax (left hemithorax)?
Cases 46-50: Drainage, Thoracotomy in Fibrothorax
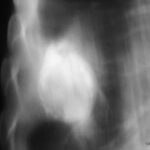
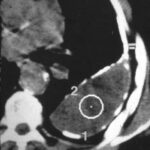
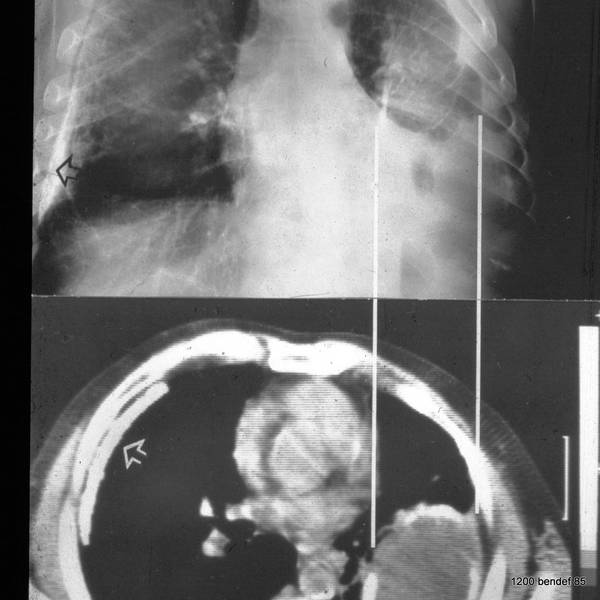
Above: Persistent effusion between both calcified pleural layers. Personne discovered: It can be reactivated in a few weeks or years, possibly only after many years. Only slight calcification of the parietal pleura; but it is present. There is no indication that the parietal pleura could not be calcified.
(Below: additionally and new, a pneumonia.)
Patient from Image 44 and 45
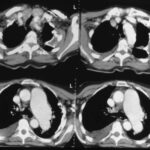
Image 46:
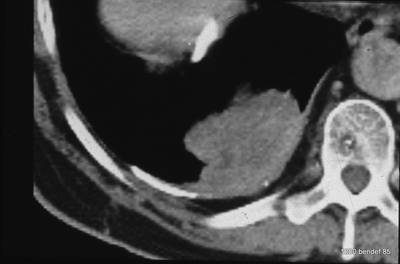
Aspiration of the Chronic Empyema. What method should be used to determine whether the persistent effusion is infected? What is the best position for the patient?

Puncture.
It is performed in the prone position. We see the image rotated to the supine position. The needle direction avoids the major vessels. Protein-rich fluid was found, and bacteriology was negative.
Reminder:
Imaging does not provide answers to the bacteriology of persistent effusions. Despite decades of sterility, the effusion can suddenly become infectiously activated without a morphological indication.
New patient 47:
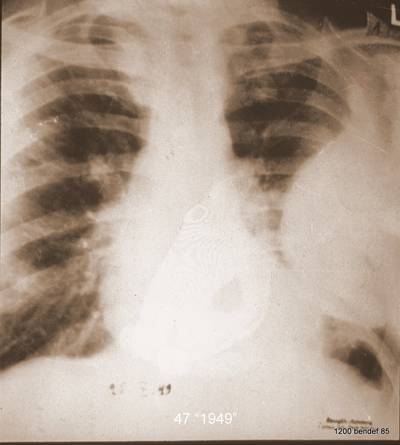
Many years ago, in 1958, this case was published in the “Tuberculosis Doctor.” The author, HG Schmitt, would be over 100 years old today. He first saw the patient in 1944.
The man was 38 years old at the time. The old X-ray (in low-KV technique) shows no calcifications.
Image 47: This patient marked the beginning of H.G. Schmitt’s interest in pleural pathology. What (incorrect) diagnosis was likely made first?
A neoplastic mass was suspected. Your answer is correct.
The technical criteria of this image are no longer allowed today. Imagine that this X-ray was taken with 60 kV. Very unfavorable for radiation protection. –
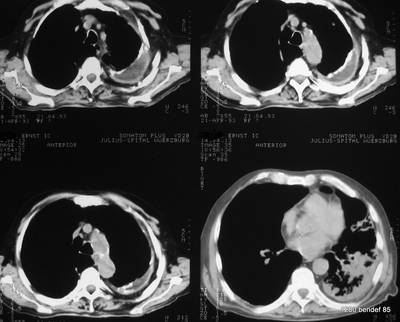
The next image shows a simple method that provides new information.
Superimposed “Target image”, 120 kV and Bucky-Potter grid – quite unusual at the time – show a large, homogeneous, spherical shadow surrounded by a calcified shell. The grayscale is inverted.
Image 48: What investigations would we order today?

Ultrasound and CT. Both procedures did not exist at the time. They would show a chronic, persistent effusion, limited by calcified visceral and parietal pleura. Note the non-calcified layer between the parietal pleura and the inner chest wall.
In 1953, they performed the following examination:
Image 49: A conventional axial tomography. What is visible?
A medical history curiosity. We see the spine, the descending aorta, the heart shadow, and the voluminous persistent effusion, surrounded by a calcified layer. The next image shows the X-ray of the surgical specimen.
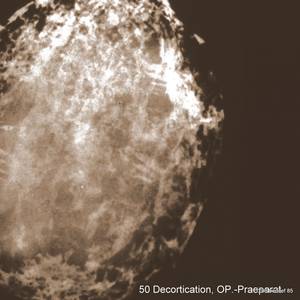
Image 50: Surgical specimen with the shell of irregularly calcified connective tissue.
Cases 51-55: Misconceptions Regarding the Pleura
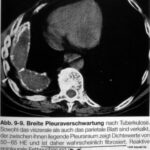
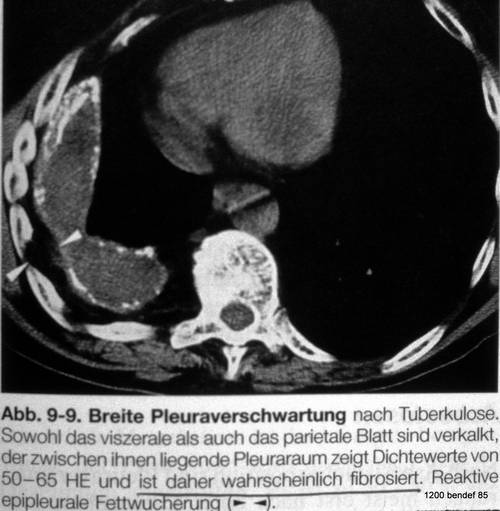
Image 51 comes from one of our current textbooks.
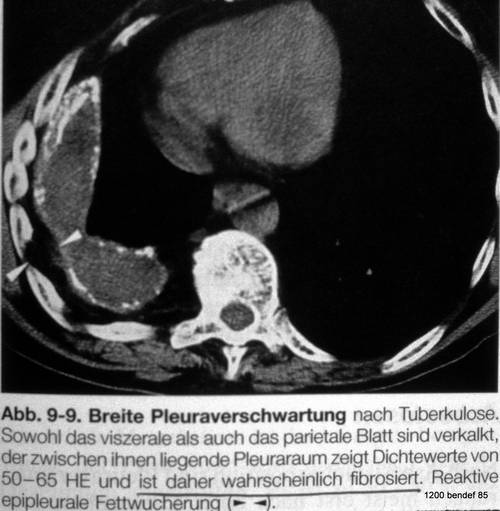
On one side, the calcifications of the parietal and visceral pleura were correctly described.
However, the space between the two pleural layers is described as “probably fibrotic” because the author took “measurements” between +45 and +60 Hounsfield Units (HU).
It is uncertain whether densitometry in a scan with artifacts (heart and respiration) and in a region so close to bony structures is reliable. – Nevertheless, this rather high density does not argue against fluid.
The diagnosis of “probably fibrotic” is nonsense.
Important findings like
– Heart displacement,
– Volume reduction of the right thorax,
– Rib pathology
are not described.
(See literature on densitometry.)
Pleural calcifications are not a harmless residual finding when – as here – an underlying effusion is associated with them. Personne’s long-term observations of persistent effusions with calcified pleura show that in 66 of 72 patients (91.2%), fistulas developed that communicated with the bronchial system or penetrated the thoracic wall.
Another worldwide misconception concerns the non-calcified layer between the parietal calcification and the inner chest wall. Many books interpret this as the parietal pleura, leading to the assumption that the parietal pleura cannot calcify, while the visceral pleura can. This is nonsense. It leads to a misunderstanding of the anatomy of both pleura. The former (or persistent) pleural space is mislocated. –
Note: Both pleura can calcify.
Image 51: Misconception. “Probably fibrotic” tissue between both pleura from a textbook.
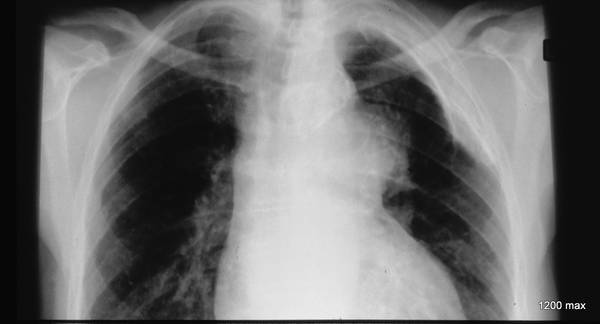
New case (52) of a 56-year-old man with bilateral tuberculous pleuritis 26 years ago.
The PA image shows a simple calcified fibrothorax on the right side. There is no fluid separating the two pleural layers, as these either adhere to each other by fibrous adhesions or simply lie side by side, separated by a thin, non-calcified layer.
On the left side, there is a strikingly thick shadow with calcification of both the medial and lateral edges. Signs of a persistent effusion include the unusually thick shadow in the pleura area, the presence of two calcified pleural layers, and the formation of a cavity instead of a complete obliteration of the pleural space.
Image 52: The very suitable case to understand the problems of both pleura

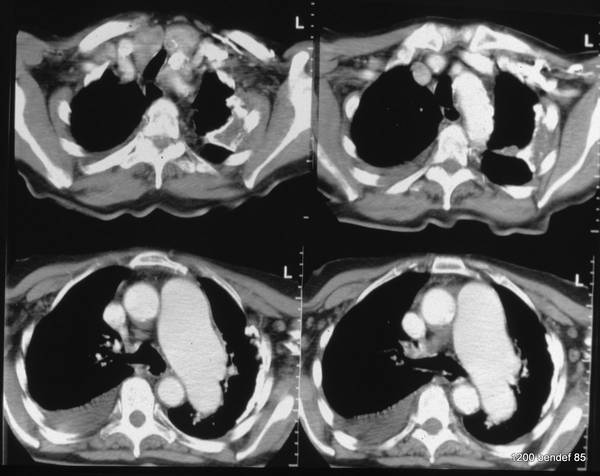
Image 53: CT of the same patient. Residual empyema (“cavity”) in the left hemithorax,
simple calcified fibrothorax without a cavity in the right hemithorax

The CT scan of the patient in case 52 shows a large, spherical fluid collection, confined to the left pleural cavity. Both pleural layers are thickened and partially calcified. The density within the cavity (+34 HU), the homogeneity, and the lack of contrast enhancement suggest that the fluid is protein-rich. Do not overestimate the absolute HU values (artifacts visible near the heart and aorta). The non-calcified layer between the inner chest wall and the calcified parietal pleura shows absorption values of –80 to –100 HU, indicating that it might be rich in fatty tissue. This layer allows for some breathing movement.
Image 54: The same patient. Synopsis of X-ray (52) and computed tomography (54)
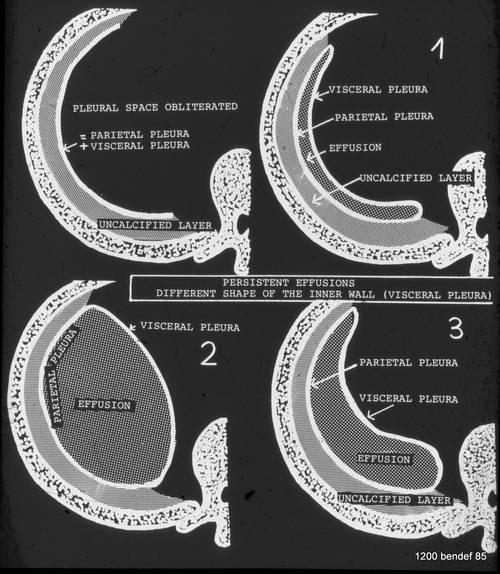
The shape of a residual effusion/chronic empyema is determined by the amount of its content.
In simple calcified fibrothorax, both pleural layers are adjacent (whether they are fused or not). In the case of a persistent effusion, the pleural walls are separated. The boundary of the inner wall (visceral pleura) is determined by the volume of the effusion (1-3).
Simple diagnosis: A large content leads to an inward-curved visceral pleura (2), as shown in images 52-54. –
The next case shows an outward-curved visceral pleura.
Image 55: The amount of fluid shapes the visceral pleura
Cases 56-60: Fluoroscopy and CT for Diagnosis
The diagnosis is not easy. The situation is as follows: On the PA chest X-ray, we see two or three lines running parallel to the chest wall. One line is typical of a simple pleural adhesion.
Remember: “More than one” line is suspicious.
This 30-year-old man (case 56) presented with dyspnea. Nine years ago, he suffered a penetrating chest injury and was repeatedly hospitalized with bloody effusions in the left pleural cavity. The drainage therapy was not adequately performed.
In the last 5 years, the diagnosis of a “calcified fibrothorax” was mistakenly made based on standard PA images. The pleural shadow is unusually thick for a simple fibrothorax and contains several axial lines. These are an indication of a persistent mantle-like effusion. A pleural puncture at a depth of 5 cm encountered resistance. Beyond this depth, a clear, protein-rich fluid collection was obtained; it was partially replaced by air.
We know two lines running parallel to the inner chest wall. Where does this mysterious third line come from?
What is the horizontal line between the two points?
How thick is the cavity?
What is the opacity?
Image 56: “More than one” line is suspicious. What is the third line?
Fluoroscopy revealed that the third line was much more of a dorsal structure (3 in the next image). It is the projection of the tangential folding of the parietal to the visceral pleura.
As a result of the puncture and the partial filling with air, there is a partial seropneumothorax.
What could be a summary of this educational case?
Image 57 (labeled and explains image 56):
Image 57: explains 56
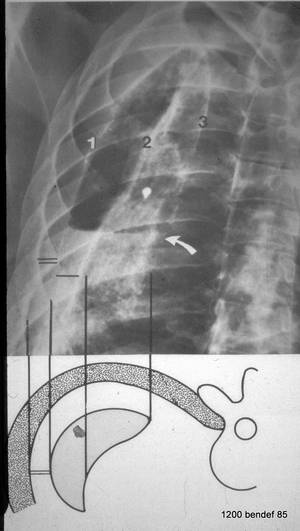
- Pleura parietalis
- Pleura visceralis
- Dorsal fold of the parietal to the visceral pleura
Single bar: Thickness of the cavity.
Double bar: Non-calcified layer between the parietal pleura and the chest wall.
The fluid level (curved arrow in image 57) is clearly visible. The “single bar” marks the axial diameter of the remaining cavity; the double bar marks the “famous” non-calcified layer between the parietal pleura and the inner chest wall. The volume of the effusion is not as large as in images 52-54.
Image 58: New patient. What do the small dots mean? How many pleural calcified lines, how many rib contours?
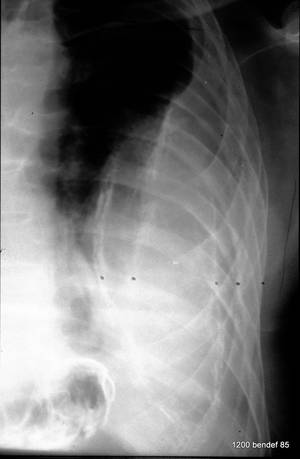
Within the large pleural shadow, three calcified lines are marked, running parallel to the chest wall. The inner and outer edges of the rib are also marked.
To continue with this patient.
Image 59: Slight rotation of the patient from image 58 towards LAO position.
What has changed in the image? What remained unchanged?
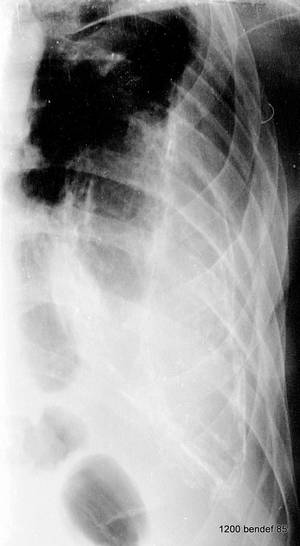
The large mass is unchanged. Also, the small, non-calcified layer within the inner rib contour has not changed.
However, there is a change in the distance and relative position of the three calcified bands.
This is a typical finding in empyemas of this form in rotating fluoroscopy. In CT (next image), it is easier to understand.
60 CT: Large effusion, surrounded by both calcified pleural layers. We understand the different results in the fluoroscopy projections:
In various LAO rotations, the parietal pleura creates only one shadow in different projections. Depending on the projection, the wavy **visceral pleura** shows different results: either two shadow lines, one, or none.
Image 60: 1 = parietal pleura;
2 = visceral pleura. Do not rely on the measured HU values of the empyema content.
The double line shows the tissue between the rib and parietal pleura.

Image 61: New case. PA chest X-ray: unclear (pleural) mass. Shrinkage? What would we do for diagnosis without a CT?
Large effusion surrounded by both parietal an visceral Pleura, both calcified.
Cases 61-65: CT and Fluoroscopy for Chronic Empyemas
Image 62: Same case: slight change in projection. – How is the patient rotated? What can we clearly see in this projection?

We see a slight rotation towards an LAO projection. It clearly shows the calcified outer and inner wall of the mass:
Classic persistent effusion with calcified inner and outer walls.
63. This new 43-year-old patient suffered a shrapnel injury 70 years ago and had a persistent pleural empyema. The process remained clinically silent. (Note: We have a selection of patients who did not reactivate.) Repeatedly, without knowledge of older X-rays, a new pneumonia was diagnosed. The history was not sufficiently investigated.
Image 63: New patient. Routine preoperative X-ray. Is it really pneumonia?

Irregular shadow, but no air bronchogram. We would like to see another projection and/or a CT scan.
Image 65: CT of this patient (66) with this small persistent empyema (with a tendency to shrink).

Image 64: This is a conventional tomography of patient 63; the patient is lying on his back and lifting his right hemithorax, reaching an RAO position. What do we see?
We see a mass surrounded by irregular calcifications; we recognize the classic separation from the chest wall. The adjacent lung is clear.
Cases 66-75: Reminder on Pleura; Long-term Observations; Fistula, Empyema Necessitatis
We leave the pleura for a moment and turn to a completely different disease. However, the same (mis)diagnosis was made, as in the previous case: pneumonia.
Image 66: The 44-year-old craftsman suffered from a respiratory infection.
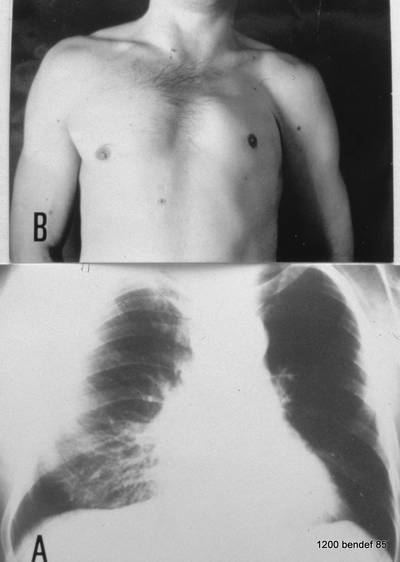
A. shows the PA film: Middle lobe pneumonia?? B. Observe the patient, not just the X-ray; this will give you the answer.
In the PA film, we are missing the (often) typical air bronchography. This means high contrast due to increased lung density, but with air-filled bronchi; bronchi are cleared by coughing and appear within the dense parenchyma as black bands or black spots, depending on the projection.
This patient does not show air bronchography but has a aplasia of the left pectoralis muscle.
Thus, his left thorax appears translucent due to the smaller soft tissue envelope. Due to this anatomy, his right thorax is slightly underexposed, simulating an opacity (no real finding).
Back to the pleura: This 74-year-old woman had pulmonary tuberculosis 51 years ago and was treated for a right-sided pneumothorax for 2 years. At age 64, she underwent surgery for breast cancer. In the last 4 years, she had three episodes of fever, and Mycobacterium tuberculosis was isolated from her sputum after repeated attempts. The X-ray from two months ago shows a voluminous pleural finding, which was incorrectly diagnosed as fibrous tissue.
Image 67: X-ray two months ago shows a huge pleural finding, incorrectly diagnosed as fibrous tissue. –
What is the calcification in the apex within the shadow just below the top of the image?
This calcified line represents the outer wall of the fluid-filled cavity! Parietal pleura. That was two months ago.
What has happened now? See the new thorax PA image in 68.
This course makes the diagnosis much easier.
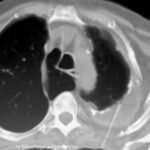
From the current X-ray, we can better understand the pleural finding in image 67: In its inner part, it is an effusion that has now been replaced by air. Spontaneously, the empyema became a pneumothorax due to a connection to the bronchial system. We do not see this pleuro-bronchial fistula, but its existence is obvious. After this drainage through the airways:
Image 68: pleuro-bronchial fistula. At this point, our patient experienced a sudden complication: Large amounts of clear fluid were coughed up. – Does part of the original shadow remain?

Yes. It is the fatty layer outside the parietal pleura, which we observe in many shrinking lesions. Such fatty layers are unusual in a healthy person.
The thickened visceral pleura was beautifully developed. –
Further sudden complications in persistent effusions are presented in images 72-75.
Image 69
Summarize the central insight from cases 67/68
A pleural shadow thicker than a finger (about 2 cm) is most likely a residual effusion. – Under such conditions, complications are often found.
An even more certain sign is the presence of more than one calcified band, indicating an effusion that separates both pleural layers.
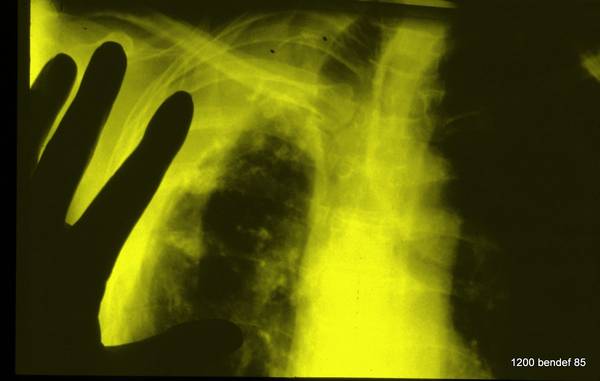
Here is a 65-year-old doctor: At age 30, he suffered from a pleural empyema; the pleura is only moderately calcified. The right thoracic cavity is restricted in the expiratory position; the ribs are thickened. He asked: Is it possible to improve my restriction?
Image 70: Chronic pleural empyema for years.

With a single diagnostic puncture, 80 ml of sterile, protein-rich fluid could be immediately evacuated. A pneumothorax could be immediately drained through the thin needle. Dense (possibly fibrinous) fluid remained on the surface of both pleural layers.
Image 71: Diagnostic puncture of this patient; seropneumothorax; thick visceral pleura
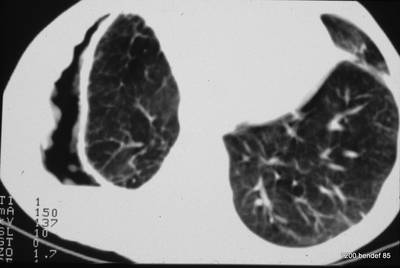
Image 72: The condition after the puncture has slightly improved (somewhat larger vital capacity); unchanged in a follow-up X-ray eight weeks later.

A year later, the finding remained unchanged in a follow-up X-ray, and the patient felt better.
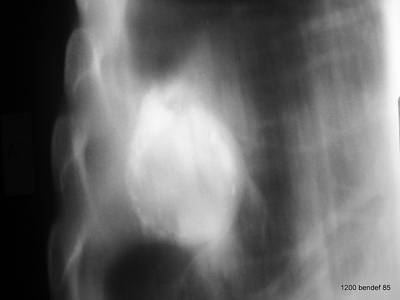
Image 73: The patient suffered from metastatic rectal cancer. Old history of tuberculosis. Diagnosis?

Persistent effusion between the partially calcified pleural layers. In fact, replaced by air due to a pleuro-bronchial fistula. Learn more about the history and click for the answer.
This 59-year-old man died from metastatic rectal cancer. A broad pleural finding, the remainder of a right-sided empyema treated 19 years ago, was always described as a calcified fibrothorax, despite significant fever and coughing that began 4 months before his death. A fistula developed, causing the contents of the cavity to be replaced by air, making it now more translucent than the adjacent lung. These findings were confirmed at autopsy.
In image 73, you see the parietal and visceral pleura as well as another line, somewhat medial, representing the connection between the two pleural layers.
There is a broad non-calcified fatty layer between the parietal pleura and the inner chest wall.
The ribs on the affected side are enlarged and marked with small black dots (12 mm distance in the middle axillary region compared to 8 mm on the opposite side). The enlargement is independent of rib alignment, orientation, or technical factors. The reasons for this phenomenon were later discussed by W. Eyler and colleagues (including W.G.H. Schmitt-Buxbaum).
The next case was complicated by a pleurodermal fistula.
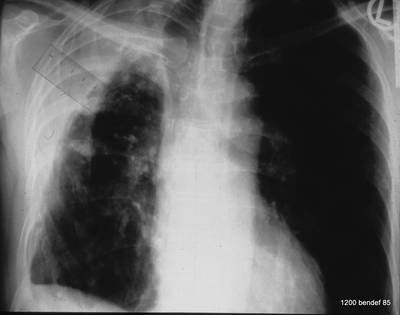
Image 74: Another complication: chronic empyema. What do we see?
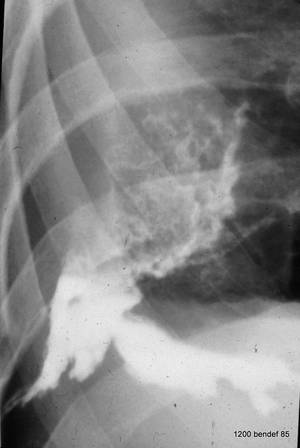
What kind of procedure was performed? What was detected?
The chronic empyema was reactivated and broke through. Pus formed a fistula that became visible on the chest wall. Filling the fistula with contrast showed the connection to the pleural cavity. The answer is: Spontaneous formation of a pleurodermal fistula. = Empyema necessitatis.
{kind=link}
{kind=link}